

Are you seeking ways to maintain a healthy smile? Do you want to know how to keep your teeth and gums healthy? If so, you’ve found the perfect blog that will answer all your queries. This post will discuss practical…

Medical Research Breakthroughs: Unveiling the Future of Healthcare
In the ever-evolving landscape of medicine, research stands as the cornerstone for advancements that propel healthcare to new heights. As we delve into the realms of medical research, we unravel the intricate tapestry of discoveries that have revolutionized patient care…

Viagra FAQ: Everything You Need to Know Before You Buy
What is Viagra? Viagra is a brand name for the drug sildenafil, which belongs to a class of drugs called phosphodiesterase type 5 (PDE5) inhibitors. Viagra is used to treat erectile dysfunction (ED), which is the inability to get or…
Pulmonary Treatment Basics: How to Breathe Better
Our breath is a vital force that sustains us, yet it’s easy to take our lung health for granted. Healthy lungs and efficient breathing are essential for our overall well-being. In this article, we’ll delve into the fundamentals of pulmonary…
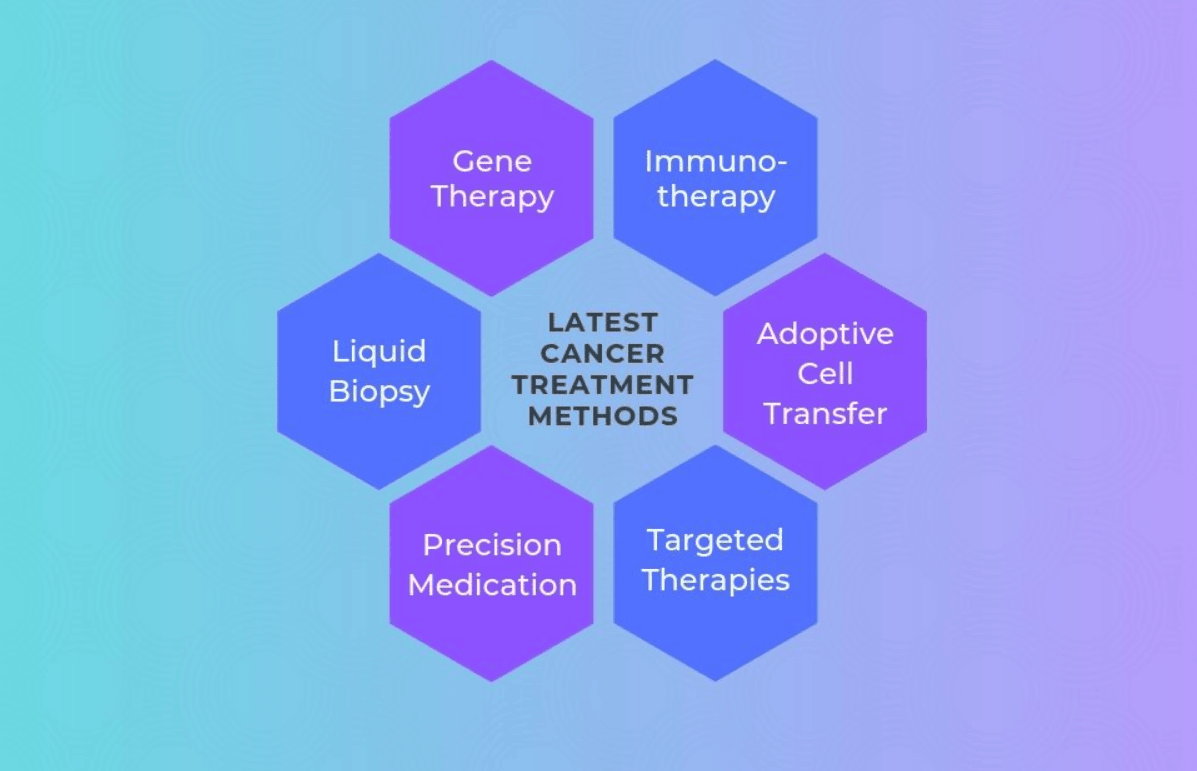
A Breakdown Of The Most Common Types Of Cancer And Their Treatment Options
Cancer is a group of diseases characterized by abnormal cell growth that can spread to other parts of the body. According to the World Health Organization (WHO), cancer is one of the leading causes of death worldwide. However, with advances…

The Latest Developments In COVID-19 Research
COVID-19, a disease caused by the SARS-CoV-2 virus, has taken the world by storm since its emergence in late 2019. The pandemic has disrupted normal life, causing widespread illness, death, and economic upheaval. To combat the pandemic, researchers worldwide have…

Understanding Anaphylaxis And How To Respond
Anaphylaxis is a severe allergic reaction that can be life-threatening. It is important to understand anaphylaxis and know how to respond to it. This article will discuss what anaphylaxis is, the signs and symptoms, common triggers, and how to respond…

How To Recognize The Symptoms Of A Seizure
Seizures are sudden and uncontrolled electrical disturbances in the brain that can lead to a range of symptoms. These can be frightening for the person experiencing them as well as for those around them who witness it. Therefore, it is…

How To Administer CPR
CPR or cardiopulmonary resuscitation is an emergency medical procedure used to revive a person who has stopped breathing or whose heart has stopped beating. Administering CPR promptly and effectively can save a life. Here’s how to do it. Step 1:…

What To Do In Case Of A Stroke
A stroke is a medical emergency that can be life-threatening. It occurs when blood flow to the brain is disrupted, causing brain cells to die. The effects of a stroke can be permanent, and recovery depends on how quickly treatment…

What To Do In Case Of A Heart Attack
A heart attack is a medical emergency that requires immediate attention. It occurs when there is a blockage in the blood vessels that supply the heart with oxygen and nutrients. This blockage can be caused by a buildup of cholesterol,…

The Importance Of Having A First Aid Kit In Your Home
Accidents can happen anytime, anywhere, and to anyone, and this is why having a first aid kit in your home is so important. A well-stocked first aid kit is a simple yet effective way to ensure that you are prepared…

Understanding The Different Types Of Medical Emergencies
Medical emergencies can happen to anyone, at any time. When they do, it’s important to know how to identify them and how to respond appropriately. Understanding the different types of medical emergencies can help you prepare for and respond to…

The Consequences Of Neglecting Health And Safety In The Workplace
Neglecting health and safety in the workplace can have serious consequences for both employees and employers. While some may view it as a minor issue, it can lead to long-term physical, emotional, and financial consequences. In this article, we will…

Why Oocytes Is Used In IVF?
Oocytes, also known as eggs, play a crucial role in the process of in vitro fertilization (IVF). IVF is a procedure in which fertilization takes place outside of the body and is used when couples are unable to conceive naturally.…

Tummy Tuck Surgery: Benefits, Preparations, Risks & More
Do sit-ups not give you the flat stomach you desire? You might be thinking of having “tummy tuck surgery,” also known as “abdominoplasty,” if you have too much fat or excess skin in your abdomen that doesn’t respond to diet…

Exercise And Diet A Couple Should Follow During IVF
To have thought of IVF, you must have gone through all the other options. Now that everything else has failed, you come to the conclusion that IVF is the only way out for you to become a mother. But if…

Which is Better for Your Skin: Profhilo Treatment vs Botox Treatment
Botox and Profhilo treatment are two popular cosmetic procedures used by many people to improve their appearance. When it comes to choosing between the two, there are a number of things that you need to consider before making your final…

A step-by-step guide to understanding the IVF procedure
In vitro fertilisation, or IVF is not a new technique. In reality, it’s a prevalent practise in Western countries, and while it’s still a long way from becoming commonplace in India, it’s come a long way. Simply said, IVF is…

What are the Different Techniques of Tubectomy?
Tubectomy, also called tubal sterilisation, is a permanent way of contraception carried out in women. In this surgical procedure, the fallopian tubes are blocked to prevent the egg released by the woman’s ovary to reach her uterus. Here’s all about…

Understanding the HSG test before you go for it
Any woman trying to have a baby should have proper knowledge about the process. It will help them in the procedure related to pregnancy. The female reproductive parts are complex and require proper functioning to perform well. The ovaries of…

Getting Your Tubes Tied: What is it All About?
Among the various forms of birth control in India, tubectomy has become quite a prevalent one. This surgical method of permanent contraception focuses on preventing the sperm from reaching the egg to fertilise it. This is done through blocking, clamping,…

Understanding The Procedure Of Plastic Surgery In Abu Dhabi
Plastic surgery is a broad genre of surgery. It caters almost to the entire human body. It is a field that demands constant creativity and diverse knowledge. From birth defects to auto-immune diseases, from cancer to degenerative ailments; plastic surgeon…

All you need to know about intrauterine insemination
If you are new to infertility treatment and wondering how you can get pregnant, then you are in the right place. Here is a guide to the IUI process or Intrauterine Insemination, which is the first line of treatment when…
Six gifts for a friend who is going through a fertility treatment
Infertility is common, which means the chances are high that you know someone who has gone through it or is experiencing it. It may be a short journey for some, while it may be long for others. But one thing…

5 mistakes to avoid during the IVF Treatment
In Vitro Fertilisation or IVF treatment is a procedure that can help couples or individuals having difficulty reproducing. It is a procedure where the eggs are collected from the ovaries and are fertilised by the sperm in a specialised environment…

The Rise of Plastic Surgery – Why More People Are Taking to the Trend
The records of plastic surgery among people right from the start Plastic surgery has many purposes today, just like the many methods and techniques employed in it. There are records of the first few applications of plastic surgery in Egyptian…

Different Pediatric Gastrointestinal Diseases and How to Deal with Them
Gastrointestinal or GI diseases in children are different from those in adults. They are more likely to suffer from general abdominal pain, diarrhoea and appendicitis. These are the main causes of hospitalization in kids. It is crucial to ensure timely…

Why and how HSG Proves Beneficial for Getting Pregnant
In your journey of undergoing infertility treatment HSG test stands as one of the most important stages, not only to determine the cause of infertility but also to increase the chances of pregnancy. You will find women claiming such on…

The fascinating world of mesotherapy- a basic guide to understanding how it works
A technique initially practised to reduce ain in the year 1952, Mesotherapy, in the current day, is known to be a technique to tighten skin and get rid of excess fat as well. This technique is seen to use injections of…
Why Do You Need Fetal Medicine During Pregnancy?
The maternal mortality rate in India per 1,00,000 live births in the most recent year, 2017 was 145, according to The World Bank data. Although the rate has fallen over the years preceding 2017, high-risk pregnancies still pose threats to…

Understanding HSG Test Procedure
Hysterosalpingography or HSG Test procedure is a test that determines the structure and shape of the uterus and examines for any kind of blockage in the fallopian tubes. The fallopian tubes are a very important part of the reproductive system of the…

Understanding HSG test and its importance
An HSG test or Hysterosalpingogram test allows your doctor to examine the inside walls of your fallopian tubes and uterus. The procedure is minor, and it gives information about the contour and shape of the uterus and detects the presence…

Uterine Fibroids: Symptoms, Diagnosis and Treatment
Uterine fibroids are non-cancerous growths. They are usually made from smooth muscle cells and fibrous connective tissues. Studies say that 70-80% of women will develop the condition at least once in their lifetime. These tend to appear in the uterus…

6 IVF Facts You All Should Know
Infertility treatment or IVF, has completely transformed the prospects for pregnancy. And it’s becoming increasingly common: approximately more than 8 million infants have been born with IVF or some other assisted reproductive technique since 1987. However, IVF is not a…

Assisted Reproductive Technology (ART) – a valuable gift from modern science
ART stands for Assisted Reproductive Technology. It refers to the infertility treatment that a person goes through to achieve pregnancy. It involves a number of treatment methodologies and should be used by people who have already gone through other processes…

4 Ways to Take Care of Premature Baby Care at Home
Premature babies are babies born before the completion of thirty-six weeks in the mother’s womb. Since it is premature birth and appropriate time is not consumed, the organs of these babies are not fully developed. Also, their immune system is…

Everything You Should Know About Preconception Care for Safe Pregnancy
How beneficial it is to have preconception care if you are trying to get pregnant? Most couples think about it today. It is essential for safe pregnancy and a healthy baby. Anytime is not too early to start preconception care,…

How do child specialists help in physical and mental development?
Bringing up a child with good habits and new learnings every day is perhaps the toughest job for the parents. Furthermore, the constant physical, mental, emotional, and other developmental changes that take place each day does not make it any…

Super amazing normal delivery tips you will ever find on the internet
One of the best experiences in a woman’s life is giving birth. It is perhaps the most natural experience a woman can have. However, the joy of being a mother is often spiked with the speculations of the kind of…
Dental Braces: What are they, and how are they done?
Dentists use wire-based appliances called dental braces to correct crowded and misaligned teeth and jaws. Many people who require dental braces do so during their adolescent years, but braces can also benefit adults. The purpose of dental braces is to…

Coronavirus and safety measures for pregnant women and childbirth: FAQs
There are many things that we are still learning about the coronavirus (COVID-19). In this article, we address some of the frequently asked questions about coronavirus and pregnancy. We have also enclosed some coronavirus safety tips for pregnant women and…

5 Questions You Must Ask Your Gynecologist Before Labor and Delivery
Pregnancy comes with many happy emotions built into it. However, women often have loads of questions especially if it is their first delivery. The top gynaecologist in Delhi also talks about bodily changes which you might face down the line.…

What is Cardiovascular Nursing?
Cardiovascular diseases take away roughly 17.9 million lives each year which includes coronary heart disease, blood vessels disorders and rheumatic heart disease, according to an article by World Health Organization. The key risk factors include diabetes, poor diet, high blood…

5 Things Your Skin Is Trying To Tell You
Your skin is literally the mirror to your health. It is the largest organ in the body and it is often the first indicator of underlying medical problems that you have not yet discovered. This article discusses 5 instances when…

Discussing the Most Common Female Medical Issues This International Women’s Day
Women have always been the pillars of strength and life-giving nurturers. Even after playing an imperative role in society consistently, most women take themselves for granted. While they take care of all the family members, they often forget to pay…
Planning to Conceive? Know What Lifestyle Changes You Need to Make this Women’s Day
Women are blessed in many ways, and giving birth to a new life is one of these blessings. But in many cases, women have infertility and the incapability to give birth to a child. In such a situation, a woman…
Looking to get treated at the best IVF clinic in Delhi? Here’s how to choose one!
If the next step in your life is to get pregnant, then you should look for all possible options. This includes looking for the fertility clinic in Delhi. There are several reasons a fertility clinic might be a smart choice. Suppose you are…

Don’t Be A Worry Wart: Undergoing Wart Removal Treatment In Dubai
Just like acne and pimples, warts are annoying and ugly to look at. They can appear anywhere on the skin, from the hands and feet to even between the toes. Though most of them are harmless, others might be sore…

When does your child need a pediatric allergy specialist?
Children are more susceptible to allergies. While some allergy symptoms are benign and can be treated at home, others may signal for a pediatric allergy specialist’s attention. In this article, we will take a look at some of the symptoms…

Reasons Why Your Baby Might Be Admitted in the NICU
New-born babies are sometimes admitted to the neonatal intensive care unit (NICU) if they are prone to any health issue like an infectious disease. You may not see it coming but there is nothing to worry about. In these cases,…

What to know about Ventricular Septal Defect
Congenital heart disease affects 0.8% to 1.2% of live births globally. Ventricular Septal Defect is one of the most common CHDs marked by structural abnormalities. It accounts for 20% to 30% of all inborn cardiac issues. Septal defect is basically…

5 Things Your Gynecologist Wants to Tell You Before Birth
Most pregnancies reach full-term without complications. However, a woman could be at a risk of UTI, preeclampsia, premature labor and gestational diabetes. Further, a mother to be can also experience mental health conditions like sad mood, appetite changes, feeling of…

Cause and Symptoms of Low Birth Weight in Newborns
In India, 25% to 30% newborns have low birth weight. Globally, there are about 20 million cases of the same annually in developing countries. It is associated with a wide range of both short-term and long-term consequences, including hearing and…

Should You Experiment With Permanent Hair Removal?
There is scarcely a person in the world who doesn’t wish to wear whatever they want and sport skin that is smooth and free of hair. But how many women are fortunate to have scanty hair growth that is barely…

When is a Hysterectomy Recommended by Gynecologists?
In India, 6% women aged between 30 and 49 years have a hysterectomy. The percentage is higher in the 45 and 49 age group. This is a minimal access surgery which is categorized into partial, complete and radical hysterectomy, along…

When is an ICSI Treatment Recommended?
Intracytoplasmic Sperm Injections were introduced to treat male infertility. It helps men father a child genetically without adoption or working with sperm donors. This assisted reproductive technology has an exceptional success rate of 80-85% and is just as effective as…

Get Party Ready With Our Style Guide
The year 2020 is drawing to a close, and the festive season is right around the corner. You must have received invitations to parties and gatherings already, and you may have planned a few parties at your house as well.…

In vitro fertilisation: all you need to know about the magic treatment
Congratulations on planning to bring a new human to this world through planned pregnancy and IVF! And, do not worry. If you are wondering what to expect when you first visit the doctor, you can relax. This article will help…
5 Questions You Must Ask Your IVF Doctor
Even after 43 years of existence in 2020, IVF is still quite a debatable assisted reproductive technology. More than 8 million children have already been born, and 2.5 million cycles are performed annually across the globe. Yet, couples tend to…

Third Trimester of Pregnancy? It’s Time to Choose Your Baby’s Pediatrician
The third trimester is usually a mix of emotions. While you reminisce about the journey to motherhood, it is only a matter of time before you welcome the child. You are already thinking of baby names and making changes to…

Suddenly Developed Body Odour? Read This
The human body is a thing of wonder. It responds immediately to how you treat it. While a person who exercises regularly and maintains a healthy lifestyle will have a toned, fit body with minimal health issues, a person who…
How to Protect Unborn Child Against Delhi’s Air Pollution?
UNICEF has declared that pollution can affect babies even before birth, impacting their growth in the womb. In fact, risk of premature birth or low-birth weight are heightened due to air pollution. Mothers who are exposed to toxic air are…
How to Have a Healthy First Trimester
Expecting a child can be a rollercoaster of emotions. The transition to parenthood is marked by several physical and hormonal changes in the body. As exciting as it sounds, this is also the time when the mother-to-be and the baby…
Understanding infertility treatment: Identification and treatment options at a clinic
Female infertility is a common problem seen globally. In fact, female infertility solely accounts for nearly one-third of infertility cases. Ideally, couples in Hyderabad must seek help for infertility after consistently trying for a year. However, at times you may be hesitant to…